by Dr Nozer Shariar
Past Secretary General & Chairperson, MTP Committee,
Federation of Obstetric & Gynecological Societies of India (FOGSI);
Past President,Mumbai Obstetric & Gynecological Society;
Member, Technical Expert Committee,
Ministry of Health & Family Welfare,
Government of India;
Member, Board of Directors,Ipas & C3 India
Member, Medical Advisory Panel,Family Planning Association of India
Presentation to:
7th Annual Mifepristone Meeting, Gynuity Health Projects,
New York, 8-9 June 2015
Point
Obtaining medical abortion without prescription from pharmacies is illegal, risky & condemned by the establishment.
Counterpoint
Obtaining medical abortion without prescription from pharmacies is a reality, a practical necessity & is used widely by women.
Traditional demand for medical methods
(Iyengar & Iyengar, RHM 2002
|
 |
Retail pharmaceutical distribution in India
(Langer & Kelkar, Biopharm Int, India Today, 2008 Nadda, Quoted in Ind Med Times, 2015) |

|
|
Year |
Mifepristone 200mg |
Combi-packs introduced: mifepristone + misoprostol |
|
|
2002 |
1.24 million tablets |
|
|
|
2009 |
15.25 million tablets |
|
|
|
2010 |
16.29 million tablets |
2010 |
1.1 million |
|
2011 |
13.76 million tablets |
2011 |
3.8 million |
|
2012 |
14.32 million tablets |
2012 |
6.8 million |
|
2013 |
11.82 million tablets |
2013 |
8.3 million |
|
2014 |
11.29 million tablets |
||
Provision of abortion by FOGSI members
- FOGSI membership in 2015 – 31,282 members
- If responsible for the over 12 million abortions annually
- Would demand an impossible 366 abortions from every estimated FOGSI member-provider annually
(Elul, Sheriar, Anand & Philip, J Obs Gyn India, 56(4):340, 2006)
Introduction of medical abortion in India
Date of approval – February 13, 2002
- Indication – For medical termination of pregnancy through 49 days of pregnancy
- To be sold by retail outletson the prescription of a gynaecologist only
- To be used only under supervision of an expert & in a hospital where back up facilities are available for blood transfusion & MTP
(Drug Controller of India, Govt of India, 2002)
Local market availability of medical abortion
- Interviewed 591 pharmacists in 60 local markets
- Returned to 359 pharmacists with undercover patients
- Pharmacists reported sales in 83.3% & undercover patients availability in 86.7% local markets
- Availability was almost universal in city & town areas but lower in rural areas
- Medical abortion dominated by combination packs
- Traditional or alternative drugs offered to 20.6%
- Median price of combination packs was Rs. 350 ($ 5.60)
- Highest in town areas – median Rs. 397 ($ 6.60)
- Lowest in rural areas – median Rs.150 ($ 2.50)
(Powell Jackson et al, PLoS One, 10(3): e0120637, 2015)
Gap between knowledge & practice among pharmacists
- Pharmacists (67.3%) knew to ask the timing of the LMP
- But only 38.5% did so in practice
- Pharmacists (35.3%) knew to ask for a prescription
- But only 13.8% did so in practice
- Pharmacists (90.9%) knew heavy bleeding was a warning
- But only 49.5% gave advice on this matter
- Pharmacists (68.0%) knew how to use a combination pack
- But only 35.3% offered the correct advice in practice
- Pharmacists (96.7%) knew where to get care for complications
- But only 28.4% gave such advice
(Powell Jackson et al, PLoS One, 10(3): e0120637, 2015)
Why the market for medical abortion is so vibrant
- Supply side
- Regulation of pharmacists & medical abortion is weakly enforced
- Few pharmacists requested to see a prescription
- Demand side
- High proportion of women want an abortion by the time they reach age 30
- Strong preference for aborting at home
- Cost of medical abortion is lower than surgical procedures.
(Powell Jackson et al, PLoS One, 10(3): e0120637, 2015)
Self-medication with abortion pills: a critique
- Retrospective observational study – 128 cases
- Self-administered of medication in 40 (31.25%)
- Presentation
- Excessive bleeding in 31 (77.5%)
- Severe anaemia in 5 (12.5%) & shock in 2 (5%)
- Incomplete abortion in 26 (62.5%) & failed abortion in 9 (22.5%)
- Management
- Evacuation in 27 (67.5%) & transfusion in 5 (12.5%)
- Strict legislation to monitor & restrict the sales over the counter with access only through approved centres.
(Niveditha & Shanthini, J Clin Diag Res. 9(1), Epub 2015)
Pathways to unsafe abortion
Study of 1,565 abortion-related cases
Complications in 29%, with half having self-medicated
| Provider type | First visit | Second visit | Third visit |
| Private doctor | 23 % | 37 % | 58 % |
| Government doctor | 9 % | 14 % | 33 % |
| Nurse ANM | 8 % | 10 % | 8 % |
| Chemist shop | 47 % | 12 % | – |
Total cost of treating complications of surgical abortion four times higher than the cost for medical abortion.
(Banerjee & Clarke, Glob Pub Health, Epub 2012)
Targeting retail outlets & pharmacies to stop sex selective abortions – and the response

|


 
|
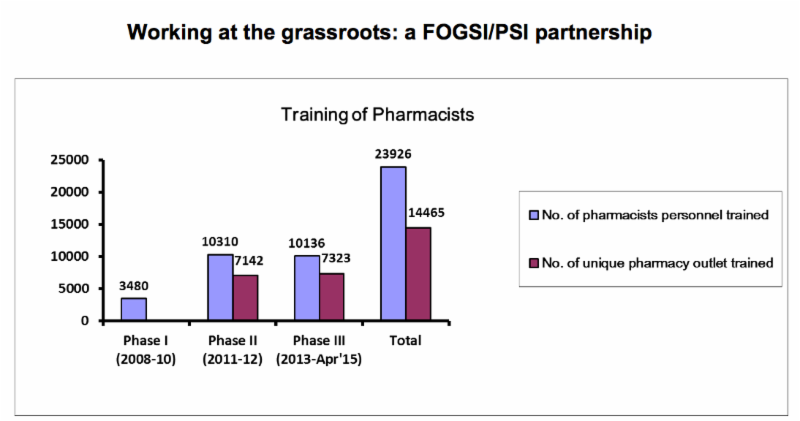
Pehel Project: Orientation for pharmacists / improvement of dispensing behaviour
(PSI India 2015) |
 |
Pehel Project: Mystery client survey
| Aggregate across three states (DL, Raj, UP) | Range | |
| Asked for doctor’s prescription |
38%
21-64%
Confirmed eligibility of women for medical abortion
94%
92-96%
Suggested correct dosage of medical abortion pills
44%
34-54%
Suggested correct route of administration
43%
26-51%
(PSI India 2015)
Role of pharmacists in expanding access
- Many pharmacists are willing to provide something to help a woman with an unwanted pregnancy.
- Women (many unable or unwilling to seek care from trained providers) already seek medicines from pharmacists.
- The specific roles of pharmacists in medical abortion will depend on a country’s legal & policy context.
- Approaches that successfully improve pharmacists’ ability & willingness to provide information as well as referrals to other healthcare providers can help & benefit women.
(Sneeringer et al, J Pub Health Policy, 33(2): 218, 2012)
Orient and sensitise pharmacists
Working strategies that are both legally compliant & situationally realistic:
- Work with pharmacists’ associations
- Impress pharmacists about their important role in supporting women’s health
- Familiarise them with the legal as well as medical issues
- Pharmacists have a responsibility to be aware of drug use
- Not wise to advocate regulatory change at this time.
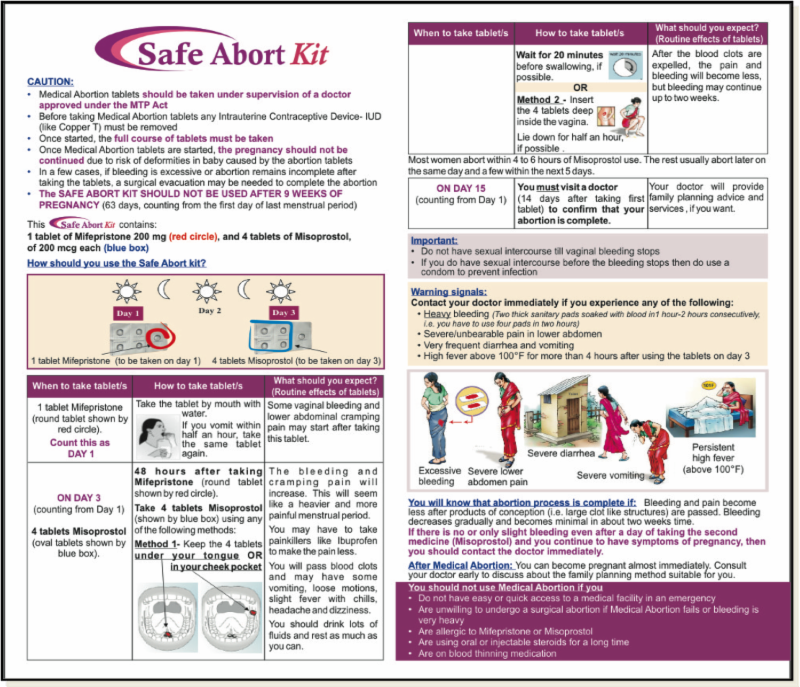
User-friendly package inserts to encourage & reiterate appropriate use
- Reiteration of appropriate dosage
- Pictorial display of mode of administration
- Assists in the early recognition of complications